This site was developed as a class project for RHBS 415 at George Mason University. Please direct comments and questions to Dr. Kevin Terry, [email protected].
Signs & Symptoms
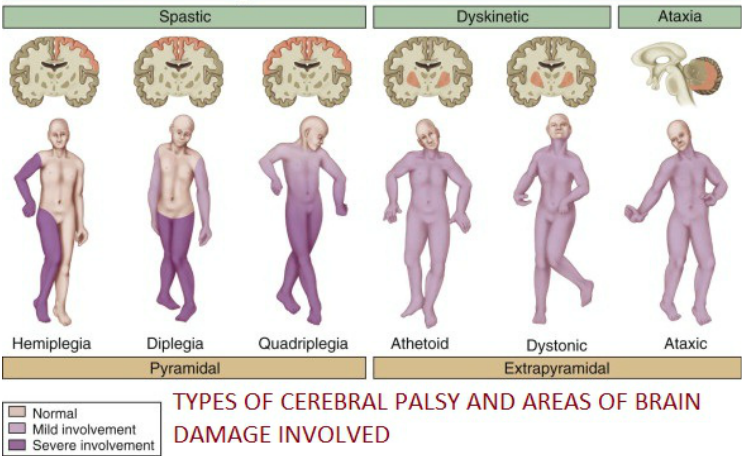
Regional involvement - hemiplegia and diplegia Global (total body) involvement - quadriplegia, athetoid, dystonic, and ataxic

Types of CP and their corresponding signs and symptoms |

|
|
Spasticity
Spasticity in cerebral palsy is defined as “a motor disorder characterized by a velocity dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyper-excitability of the stretch reflex, as one component of the upper motor neuron syndrome” [3]. Spasticity in cerebral palsy is usually measured by the Modified Ashworth Scale [13]. Most children that are diagnosed with cerebral palsy have spasticity as their main motor function symptom, which makes it difficult to move, causes pain, and creates complications during daily activities. Spasticity in cerebral palsy prevents the stretching of muscles, ultimately resulting in the slow lengthening of the bones, formation of contractures, and difficulties in fine and gross motor movements [14]. Spasticity can lead to quick muscle fatigue. Coactivation/Co-contraction Coactivation/co-contraction is defined as opposing muscles (antagonists and agonists) firing at the same time, which means they are working against each other. Coactivation/co-contraction can be positive or negative, in CP it is negative because it affects postural control during reaching and standing which limits performance. When reaching, children with CP show postural corrections that are direction dependent. When standing, children with CP have poor muscle timing and experience muscle coactivation. An example of coactivation/co-contraction in CP would be the hamstring muscles contracting simultaneously with the quad muscles, this causes a series of issues including lack of control and lack of precision due to an inability to produce proper amount of force [16]. Coactivation/co-contraction of opposing muscles also increases the energy output, meaning that the child will fatigue much more quickly [17]. Anticipatory postural adjustment development varies in children with CP compared to stable development in children without CP. Stability and alignment is greatly affected in children with CP. The study in 2011 describes an experiment involving 12 children with CP and 12 children with normal development. The children with CP and the control group were to catch a ball while sitting. It was concluded that as normally developing children age, they have an increase in anticipatory postural control and a decrease in compensatory postural control while in contrast children with CP have a decrease in anticipatory postural control and compensatory postural control [16]. Dystonia The main physiological symptom associated with dystonia, altering muscle tone, is hypertonia, otherwise known as acute muscle rigidity or stiffness [9]. This results in an inability to move major muscle groups and resistance to changes in position as well as poor balance and posture [5]. Children diagnosed with dystonia also frequently experience issues with communication due to lack of control over facial muscles [5]. Patients with cerebral palsy "demonstrated that muscle cells of the flexor carpi ulnaris of children with CP are twice as rigid as muscle cells of patients without neurological impairment. This increased muscle stiffness can contribute to atypical postures and movement problems in children with CP" [18]. They have more of an inability to recruit muscles with speed, time, and precision [18]. It was noted that muscles maintained in shortened positions demonstrate fewer series sarcomeres, a reduced length, and an increase in passive stiffness. The converse was also true when muscle maintained a length over a longer period of time, the sarcomeres increased and the muscle became longer. The problem of rigidity was the inability of the muscles to produce a transition in the muscle's length-tension relationship. The awkward transition led the muscle to be very stiff [18]. This rigid resistance can cause fatigue in individuals with CP. 
Fatigue
"Fatigue is used to describe a reduced capacity to sustain force or power output, reduced capacity to perform multiple tasks over time, and the experience of feeling exhausted, tired, weak, or lacking energy" [19]. The debilitating symptoms of CP cause fatigue in general when walking, standing, sitting, and during reaching/grasping because they require more muscle force to produce and maintain the abnormal movements and postures. When the body has to generate more force in order to maintain abnormal movements, there is a greater expenditure of energy, leading to increased fatigue. Another aspect to touch on is the efficiency of the abnormal movements, when something becomes less efficient more resources are wasted in order to get the task done. In the case of CP patients, the abnormal movements causes an increased use of energy that ultimately fatigues the patient much more quickly than if their motor patterns were more efficient. |
Contracture
Muscle spasticity eventually results in contracture, which is the stiffening and shortening of muscles. At the University of California, San Diego and Rady Children’s Hospital, researchers recruited 33 children with cerebral palsy (CP) and 19 children (control) with no neurological disorders for a study to compare the hamstring muscle biopsies of CP children with the children in the control group. The CP children were undergoing hamstring lengthening surgery involving the gracilis and semitendinosus muscles and the control children were undergoing ACL reconstructive surgery with a hamstring autograph using gracilis and semitendinosus tendons and part of the muscle [15]. One of the findings was that children with CP had substantially stiffer muscle tissue than the control children. Another finding was that children with CP had more collagen and the in vivo sarcomere length was longer in CP hamstring muscles than the control muscles. The researchers concluded that extracellular matrix stiffness and in vivo sarcomere length cause contracture, a muscular limitation in individuals with cerebral palsy [15]. Contracture results in the inability to execute motor movements and control posture as productively as a normally developing person, leading to an increase in fatigue during those activities. 
Contracture in the leg
Choreoathetosis
Choreoathetosis is defined as irregular and uncontrollable movement of the limbs and/or facial muscles [9]. This abnormality occurs when the major muscles of the limbs and face switch back and forth between states of relaxation and hypertonia uncontrollably, causing massive jerking motions [5]. This can result in drooling due to lack of control over facial muscles, inability to grip or handle objects, and varying levels of muscle spasms made worse by physical and emotional stress [5]. 
Uncontrollable hand movements inhibiting reach and grasp
Ataxia Ataxia refers to a loss of muscle coordination that happens mostly in the limbs. Depth perception and balance are affected and quick and precise movements become increasingly difficult. Ataxia also includes tremors meaning that when someone with CP is deliberately reaching for something their hand begins to tremble. This trembling worsens as an individual moves closer to an object [6]. Ataxia has been found to be associated with de novo point mutations. As part of a genetic investigation to study children with ataxia, a research team identified four patients with Ataxic CP. Each patient was found to have mutations in three different genes which were de novo and associated with increased paternal age. The mutations were shown to be pathogenic through the use of bioinformatics analysis [6]. 
Ataxic tremors
Psychosocial Effects Psychosocial refers to the behavior and mental well-being of an individual molded from social and environmental influences. Children with CP need a healthy atmosphere to grow and apply self learning techniques in. Specific behaviors that are most problematic "for children with cerebral palsy were identified as dependency, headstrong, and hyperactive” [20]. Even with strong personality, guidance from a parental figure, peer, or coach may help mediate fear and anxiety. Children who do not have strong familial support are more susceptible to anxiety, negative moods, and low self-esteem. Shown in the Figure 4 below, the CP children raised by incomplete families and CP children raised by unrelated guardianship had higher rates of psychological issues when compared to the corresponding control groups. Anxiety and fear were found to be tied with family, environment, and affection. The article demonstrated how important "upbringing type, family climate and interrelations between a child and "educator/s"' is for psychological development for children with CP. Increased familial support led to greater psychological outcomes for children with CP [20]. |
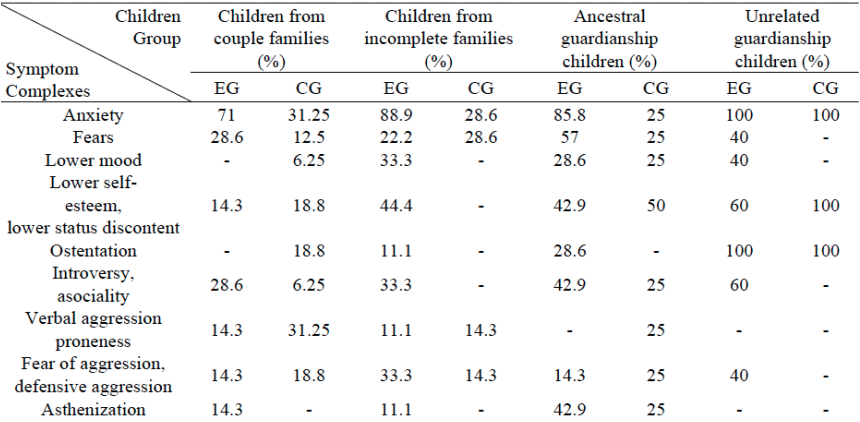
Children with CP and children without CP took an anxiety test followed by an imaginary animal drawing test. With the data, Akhmetzyanova did a comparative analysis among the population separating the children in groups of how they were raised [20]. The EG group is referring to the ‘experimental group’ being children who have CP whereas the CG group is the controlled group. The controlled group is the set of the kids that have no history of musculoskeletal disease. In Figure 4, it shows a higher level of reported fear among children raised by a couple, an incomplete and ancestral guardianship if the child had CP than those who did not. Across the board the experimental group also were higher levels of Introversy, fatigue, irritability and lack of appetite (asthenization).
EG - experimental group (children with CP)
CG - control group children (children with no history of musculoskeletal disease)
Children from couple families - children raised with two parents (mother/father)
Children from incomplete families - children raised with one parent (mother)
Ancestral guardianship children - children raised by relatives (grandparents)
Unrelated guardianship children - children raised by foster-parents (non-biological parents) [20]
EG - experimental group (children with CP)
CG - control group children (children with no history of musculoskeletal disease)
Children from couple families - children raised with two parents (mother/father)
Children from incomplete families - children raised with one parent (mother)
Ancestral guardianship children - children raised by relatives (grandparents)
Unrelated guardianship children - children raised by foster-parents (non-biological parents) [20]
Psychosocial Effects on Learning and Socialization
|
Learning
Children with CP may also have a shorter attention span and motor movement issues. The children that have to put more effort into walking and other complex movements tend to feel fatigued or overwhelmed when it comes time to learn. The moderate to severe cerebral palsy patients generally have a more severe intellectual disability [21]. 
|
Socialization
There is a strong correlation between low self-esteem and low levels of motivation. This can be contributed to being less mobile than others. A behavioral study was conducted by Ragonesi where she offered mobility assisting technology to a set of mobility impaired cerebral palsy children and compared their socialization in the classroom to those who did not use the technology. She concluded that mobility training is developmentally effective for young children "if provided under controlled, experimental conditions" to increase quality of life through social interaction and mediated behavior therapy [22]. |
Functional Limitations
|
Individuals with CP have limitations in performance mostly due to their improper gait.
Crouch Gait Muscle tightness and spasticity are associated with crouch gait, one of the most common gait abnormalities seen in individuals with Spastic CP. Crouch gait shown to the right in Figure 5, includes greater knee flexion and hip flexion that causes an individual to hunch forward. The knee and hip flexion can be the result of muscle tightness and the inability to extend the lower limbs. Crouch gait typically gets worse and can lead to joint deterioration. This type of gait requires more muscle exertion than normal gait, which can cause an increase in difficulty in walking, balance, standing, and posture, leading to an increase in fatigue [23]. |

Figure 5: Crouch gait
|
Cerebral Palsy Gait Demonstration Video [24]
